Gm final practical short case sheet
This is an online e-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Date of admission:30/07/2022.
A 45yrs old female ,farmer by occupation is a resident of nalgonda presented to casuality with the Chief complaints Of Fever and body pains, not associated with chills since 10days.
HISTORY OF PRESENT ILLNESS
Patient was apparently asymptomatic 13 days ago,then she developed fever which is sudden in onset and intermittent,it is not associated with chills and controlled temporarily on medication.
Patient complaints of dark coloured stools since 3 days(melena),body pains and joint pains since 2 days .
Also complaints of vomtings 1 episode yesterday night which was non projectile and non bilious..
history of loss of appetite since yesterday.
There is no history of rashes, burning micturition,hematuria,hematemesis,
Neck stiffness.
PAST HISTORY
There are no similar complaints in the past.
Not a known case of
TB
Asthma
Diabetes
Epilepsy
CVA
CAD etc.
PERSONAL HISTORY
Diet-Mixed
Appetite-Normal
Bowel and Bladder movements-Regular
Sleep- adequate
No Addictions either tobacco using or alcohol
ON EXAMINATION
Patient was conscious, coherent, cooperative and we'll oriented to time place and person
Moderately built.
GENERAL PHYSICAL EXAMINATION
Pallor- present
Icterus- absent
Cyanosis- absent
Clubbing- absent
Generalized lymphadenopathy- absent
Clinical examination :






VITALS**
Temperature- 101.4F
Pulse rate -80bpm
Resp rate - 16cpm
Blood pressure-110/82mmHg
sPo2 98% at room temperature
SYSTEMIC EXAMINATION
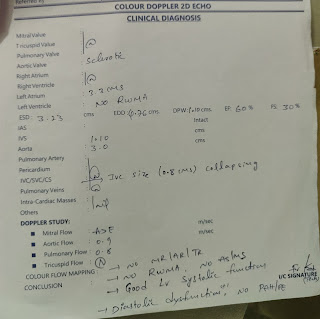
CVS: Inspection
Chest wall is bilaterally symmetrical.
No precordial bulge is seen
Palpation
JVP- Normal
Apex beat -felt in the left 5th intercoastal space in the mid clavicular line
Auscultation
S1&S2 are heard,no murmurs found.
RESPIRATORY SYSTEM
Dyspnoea- no
No wheezing sounds
Position of trachea- central
Bilateral air entry, normal vesicular breath sounds are heard.
No added sounds
CVS
Patient is conscious
Speech normal
No signs of meningeal irritating
Motor and sensory system- Normal
Reflexes - present
Cranial nerves - intact
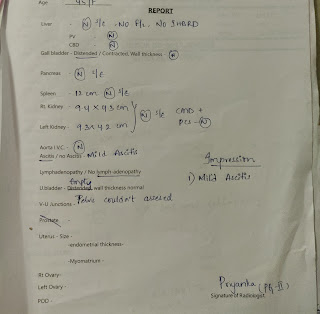
PER ABDOMEN
Liver non palpable
Spleen non palpable
Soft and Non tender.
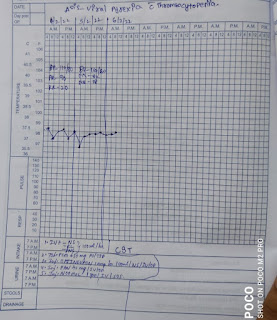
FEVER CHART
INVESTIGATIONS


Hb-11.3
TLC-1500
Platelet count-42000
Rbs-242 & Fbs- 126
Hb1Ac-6.9
Hb-11.6
TLC-2150
Platelet count-75000



PROVISIONAL DIAGNOSIS
VIRAL PYREXIA with thrombocytopenia
TREATMENT
IVF -NS,RL.DNS
Tab- paracetamol 650mg TID
Inj- PANTOP 40 mg
Inj- NEOMAL if temp rises above 102f
Inj-OPTINEURON 1mg Iv


Comments
Post a Comment